Thoracic Outlet Syndrome: Solve the "Numb Hand" Mystery
Stop treating your wrist for a problem that starts in your neck. Targeted structural decompression for the "Invisible Pinch" that standard scans miss, and massages can’t reach.
Quick Navigation: Solve the Mystery of Your Numb Hand
The 20kg "Smartphone Tax"
Brain Fog & Venous Congestion
The MRI Gap
Gilliatt-Sumner Hand
The Stress-Breathing "Noose"
The 60-Second Self-Audit
Self-Diagnosis Checklist
Is it Carpal Tunnel, or is Your Neck "Strangling" Your Nerves?
In Singapore’s high-pressure work culture, Thoracic Outlet Syndrome (TOS) is the ultimate "mystery illness." You’ve likely spent months bouncing between GPs, TCM practitioners, and massage therapists, only to be told your scans are "normal and it's "stress" or "Carpal Tunnel."
The Science
The "Why" Behind the Pain
‼️ Doctor's Note:
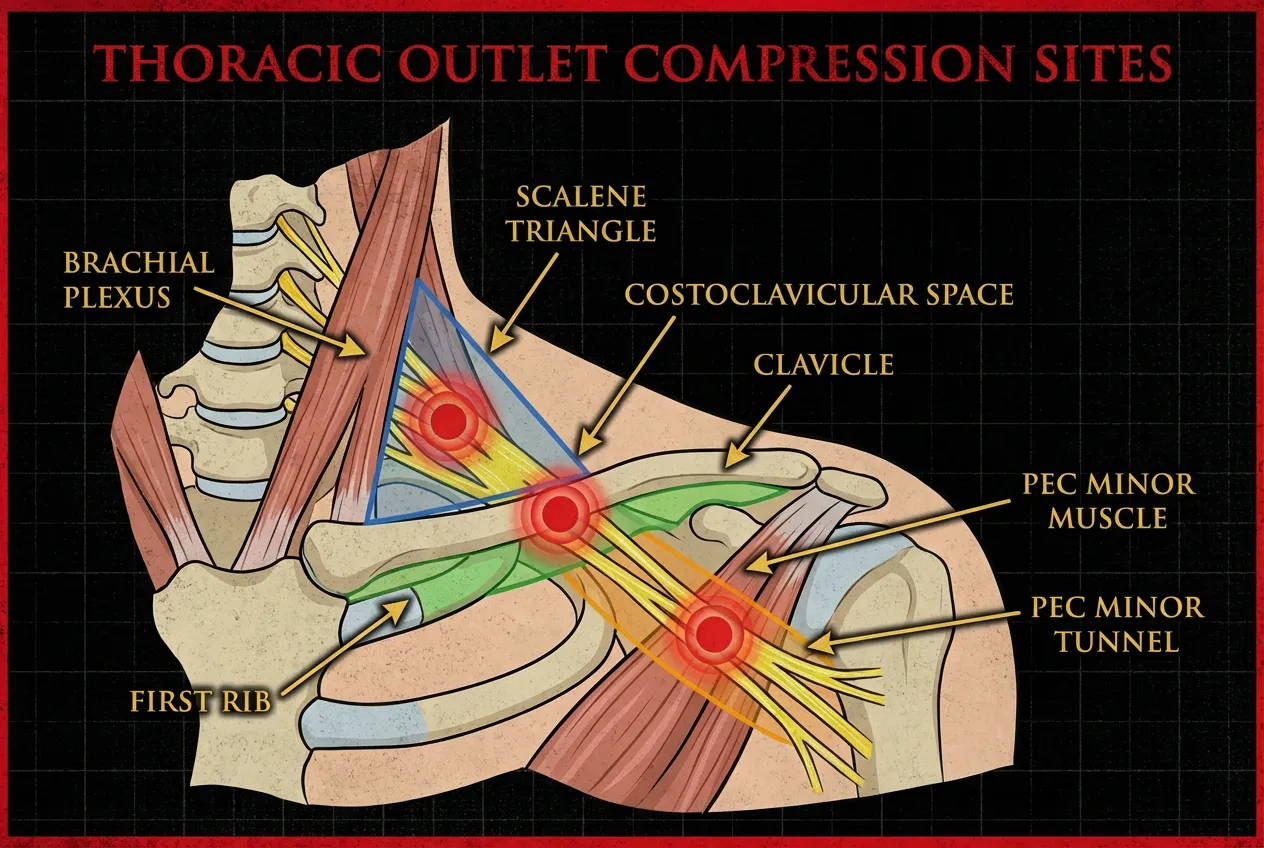
"Patients are often terrified when their hand goes numb, fearing a stroke or permanent damage. But look at the diagram. Your nerves (The Brachial Plexus) must pass through a tiny 'Danger Zone' above your first rib. If your posture has shifted from years of CBD desk work, that space vanishes. We don't just 'rub' the shoulder; we use X-ray analysis to find the structural blockage and physically reopen that tunnel."
Clinical Note
Do your headaches come with a feeling of floating, giddiness, or a spinning room? Your neck's "GPS sensors" may be failing.
The FUNCTIONAL GAP
Why Your MRI Came Back "Normal"
Standard MRIs are "Neutral Scans" taken while you are lying flat and still. But Thoracic Outlet Syndrome is a Functional Crisis.
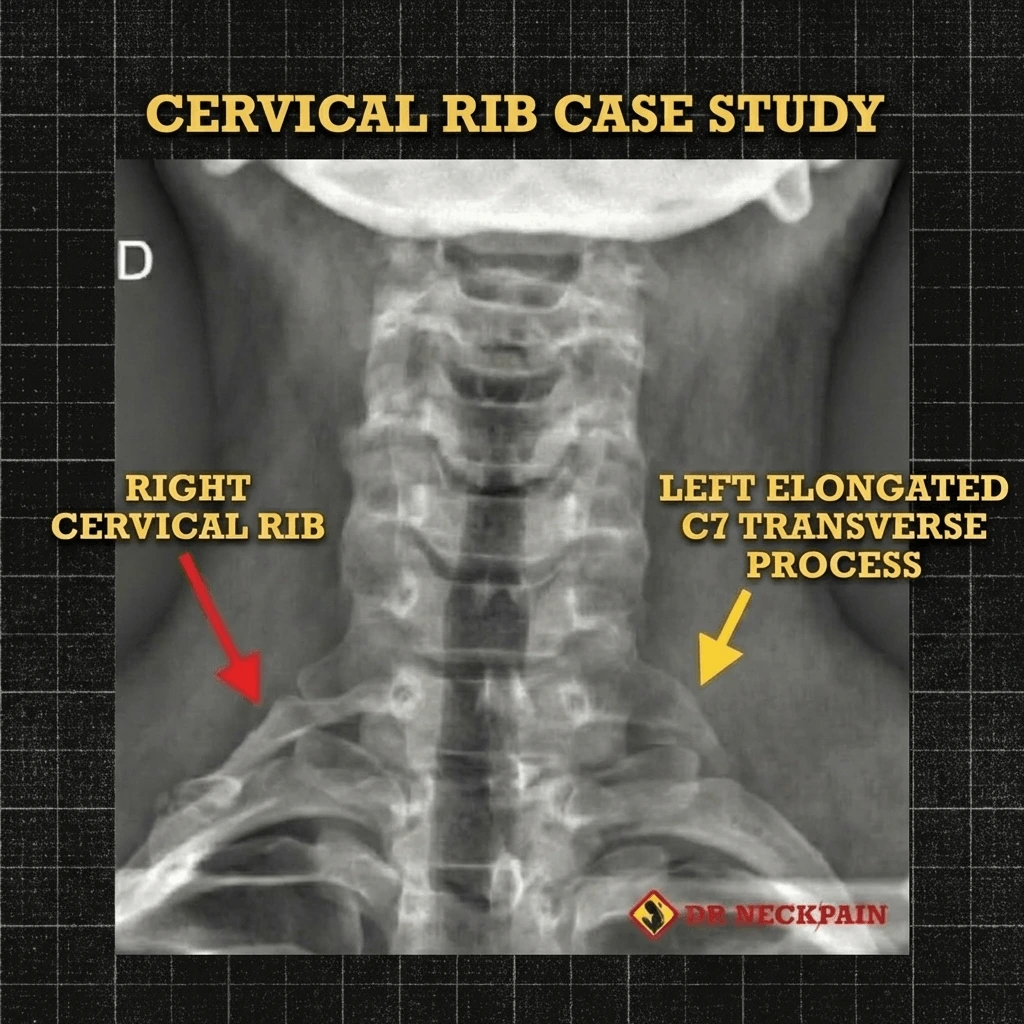
The Genetic "Nerve Trap"
Some are born with an extra Cervical Rib or the Scalenus Minimus muscle (an "accessory strangler" found in 50% of TOS sufferers).
Think of it as a rare anatomical quirk you were born with that stays "silent" until your first office job.
Once you start spending 8–10 hours a day at a desk, that dormant "quirk" begins to physically strangle your nerve tunnels.
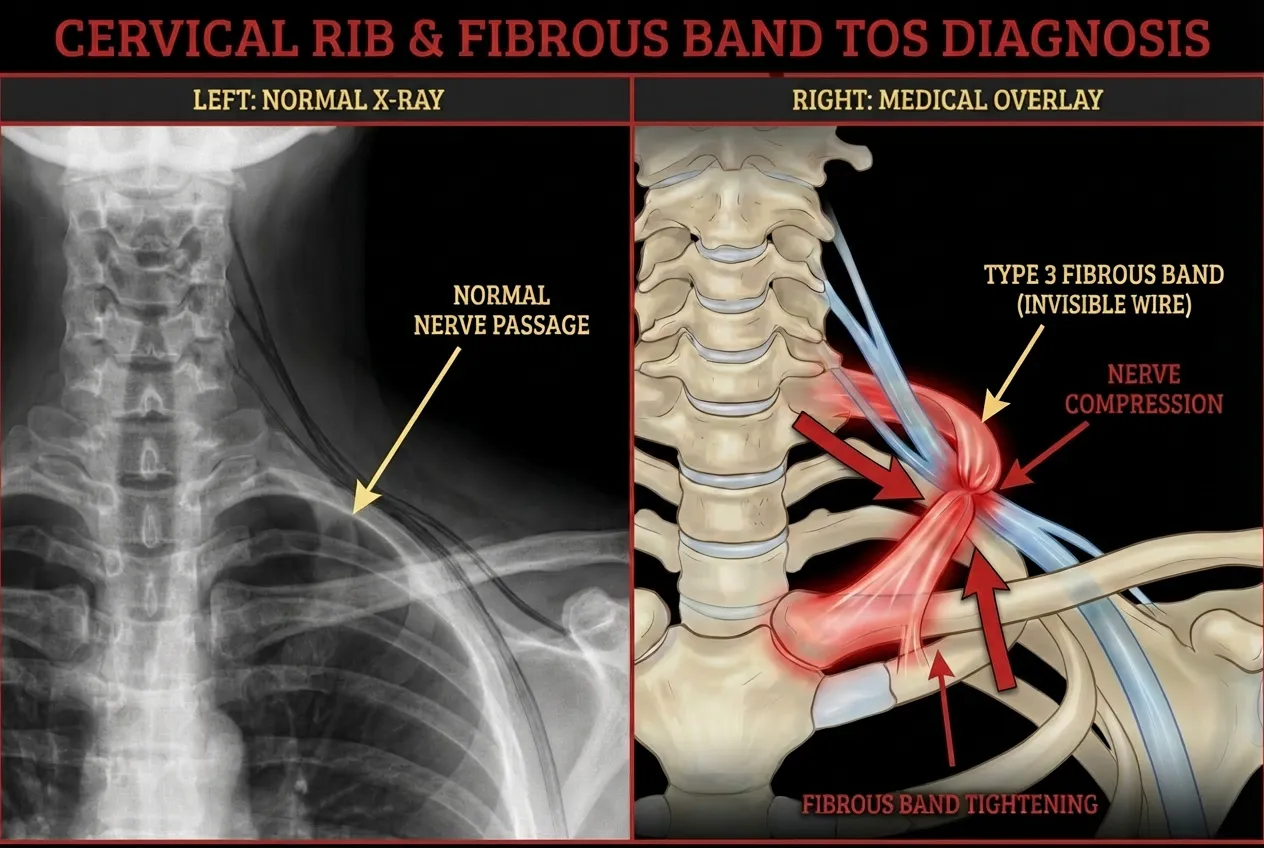
The "Invisible Wire"
A "Type 3 Incomplete Rib" or distal fibrous band acts as a snare that only tightens when you move, making it invisible on static scans.
The "Neck Hinge" Collapse
Chronic pain often stems from a collapse of structural tensegrity. Instead of a smooth curve, your neck "hinges" at a single segment. This physically narrows the "Fuse Box," triggering a protective Biological Splinting response in your muscles.
The Scalenus Minimus
(The Accessory Strangler)
Current research confirms that up to 50% of TOS sufferers possess an accessory muscle called the Scalenus Minimus. This muscle creates an extra, narrow "tunnel" that further compresses the Brachial Plexus. If you have this anatomical variation, standard stretches won't work, you require a mechanical reset to increase the outlet volume.
📱 The Digital Epidemic
The 20kg "Smartphone Tax": Why Singapore's Tech Obsession is Fueling a TOS Epidemic
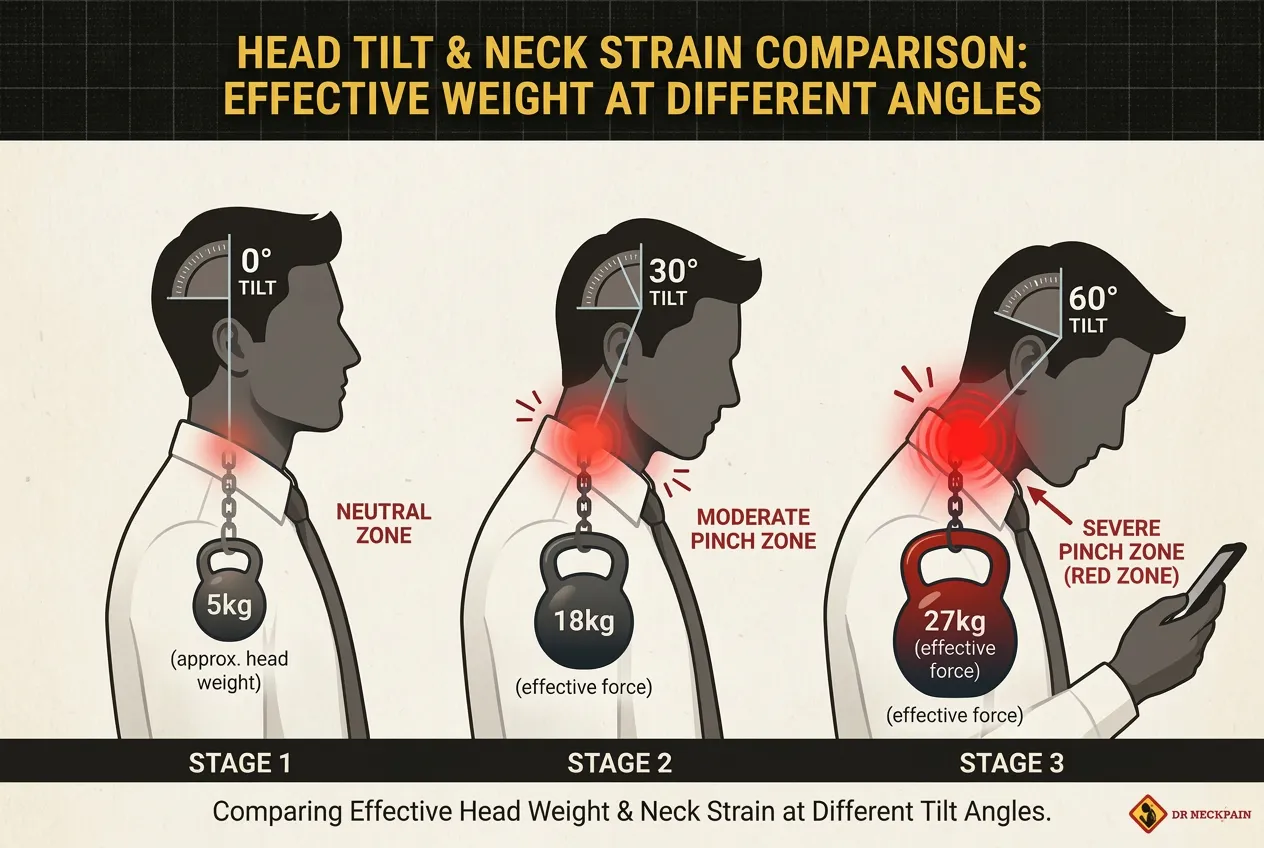
Singapore leads the world in smartphone penetration, but our digital productivity comes with a hidden structural cost. While your iPhone weighs only about 200g, the physics of leverage tells a much more dangerous story for your nerves.
The Physics of the "Invisible Pinch"
In a neutral, upright position, your head weighs approximately 5kg. However, for every inch you tilt your head forward to type an email or check Slack, the effective weight on your lower neck and Thoracic Outlet doubles.
15° Tilt: 12kg of pressure
60° Tilt (The "Text Neck" Standard): Up to 27kg of sheer force grinding down on your first rib and collarbone.
⚠️ The Result
This massive, sustained pressure physically collapses the "tunnels" that house your Brachial Plexus. This isn't just "bad posture", it is a mechanical closing of the gate. Over time, this 20kg "tax" creates the Invisible Pinch that leads to 3 AM wake-ups and numb fingers.
‼️ Doctor's Note
"Your body wasn't designed to support a 27kg weight at a 60-degree angle for 10 hours a day. We see patients who have 'perfectly normal' MRIs because the scan was taken lying down. But the moment they sit up and look at their phone, the 'tax' kicks in and the nerves are strangled."
🧠 The Hidden Symptom
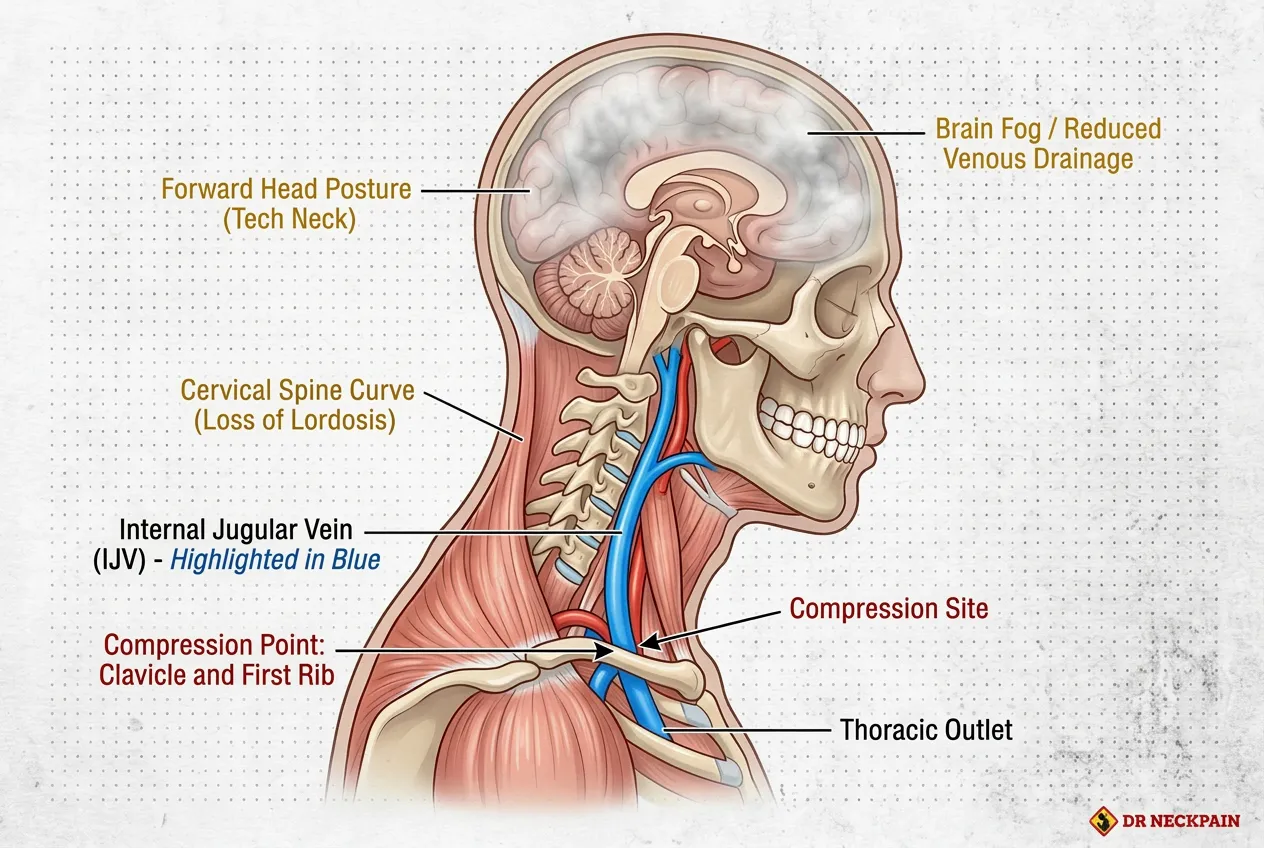
🧠 The "Brain Fog" Connection: Is Your CBD Office Job Draining Your Mental Clarity?
Most of our patients at North Bridge Centre are shocked to learn that their "3 PM Slump" and mental fatigue aren't just caused by coffee crashes. Clinical research (Jayaraman et al., 2012) has identified a direct link between Thoracic Outlet Syndrome and Internal Jugular Vein (IJV) Compression.
The "Clogged Drain" Effect
Your brain requires a constant cycle of fresh, oxygenated blood. For that to happen, "used" (deoxygenated) blood must drain out through the Internal Jugular Veins, which pass directly through the Thoracic Outlet.
When your collarbone collapses or your first rib "jams" upward, it acts like a kink in a garden hose.
This creates Venous Congestion:
The Symptom: Chronic brain fog, a "heavy" feeling in the head, and lightheadedness.
The Reality: Pressure is building up because the "drainage pipes" are being squeezed by your own anatomy.
The CBD Factor: Staring at dual monitors for 10 hours a day puts your neck in the exact position that maximises this compression.
‼️ Doctor's Note
"I’ve had patients who spent thousands on 'Nootropics' and supplements for brain fog, only to find that their mental clarity returned the moment we structurally reopened their Thoracic Outlet. If the blood can’t leave your head, fresh oxygen can’t get in. This structural restoration is a vital component of our Neck Optimisation Protocol for high-performers."
TEST YOURSELF
The 60-Second "Short Circuit" Audit: Wrist vs. Shoulder
Before you commit to wrist surgery or another round of splints, perform these two clinical manoeuvres. The results will tell you exactly where your "Power Line" is being pinched.
Test A: Phalen's Manoeuvre
(The Wrist Check)

THE ACTION:
Press the backs of your hands together firmly with fingers pointing down. Hold for 60 seconds.
The Verdict:
If you feel tingling in your thumb and index finger, the issue is likely in the wrist. If you feel nothing, your "Carpal Tunnel" may be fake.
Test B: The ROOS Test
(The Specialist Verdict)

THE ACTION:
Lift both arms up into a "Goal Post" position. Slowly open and close your fists for 60 seconds.
The Verdict:
If your arm feels heavy or you get numbness in your pinky, the issue is Thoracic Outlet Syndrome, not your wrist.
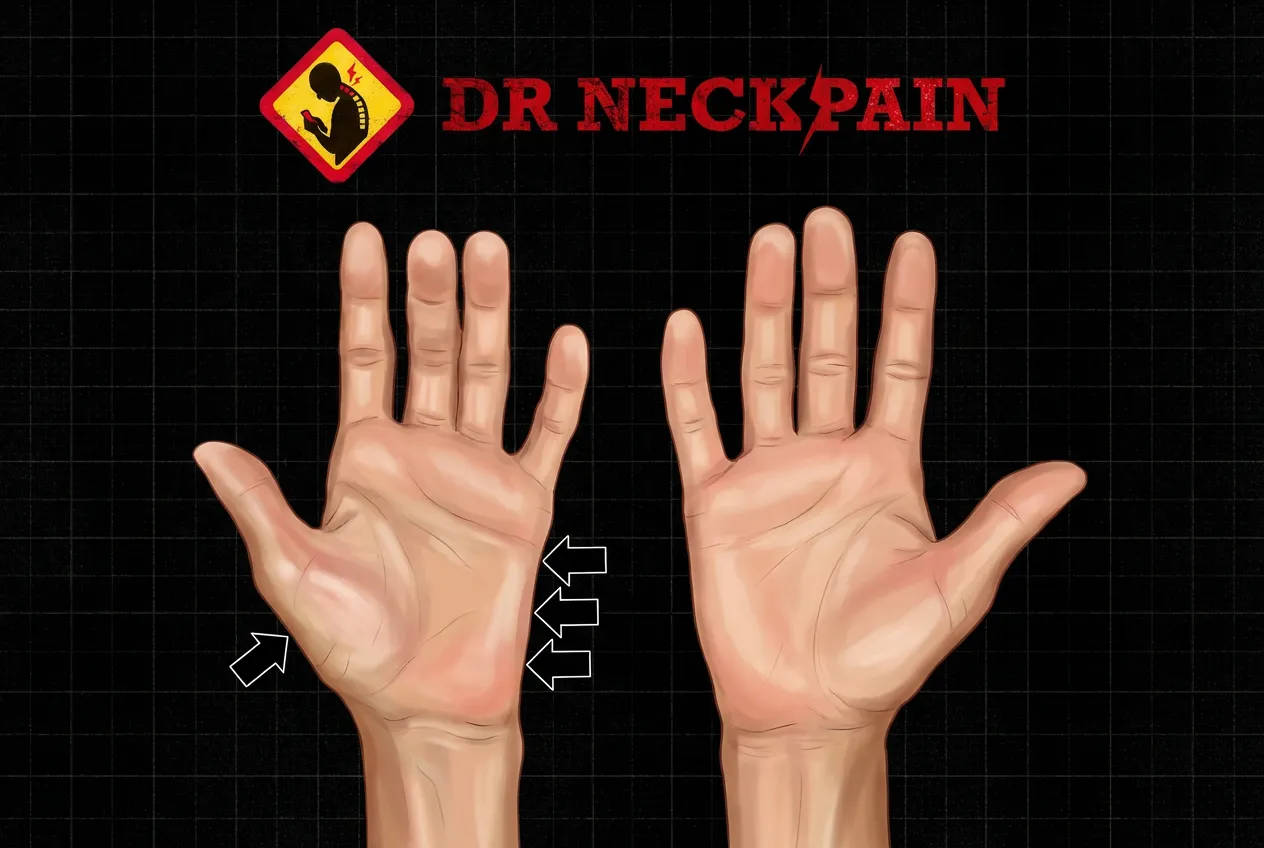
A Critical Warning Sign: Muscle Wasting at the Base of Your Thumb
Look at the soft, fleshy pad at the base of your thumb, the rounded mound on your palm. If that area appears visibly flat, sunken, or noticeably smaller than the same spot on your other hand, this is a serious warning sign, known as the Gilliatt-Sumner Hand.
It means the nerve compression has been present long enough that the muscles it feeds have begun to waste away from a lack of signal. Your Thoracic Outlet Syndrome has reached an advanced stage (True Neurogenic TOS).
‼️ The Surgical Reality
According to a 25-year clinical review in the journal Neurosurgery (PMID: 15458596), reaching this stage of muscle atrophy provides a "clear operative indication." To prevent permanent, total loss of hand function, the standard medical protocol is immediate surgical intervention (such as a first rib resection) to physically cut away the impingement or surgically decompress the brachial plexus to prevent permanent, irreversible loss of your hand's motor function.
❤️ Our commitment to complete honesty
What cannot be reversed: Once the Gilliatt-Sumner Hand has developed and that muscle tissue has visibly shrunk, the loss is generally permanent. No form of conservative care - including ours - will restore that muscle bulk. We will never suggest otherwise.
What we may still be able to help with: Muscle loss is one issue. The pain, numbness, and tingling travelling down your arm are another. Even at this advanced stage, Dr Will Kalla may be able to significantly reduce or resolve those symptoms through structural correction.
⚠️ One thing we need you to do first
Because the Gilliatt-Sumner Hand is a severe clinical presentation, our clinic policy is firm: you must first consult with a surgeon before we evaluate your case. This is not us turning you away; it is us ensuring you have the complete clinical picture before any structural work begins.
Whether you proceed with surgery is entirely your decision. But that surgical assessment must happen first, and it should happen soon - not "when you get around to it". Once you've been evaluated, contact us, and we'll discuss whether our protocols are the right next step for you.
🚨 The Bottom Line
You have a window of opportunity to fix the structural alignment of your upper cervical spine and decompress the Thoracic Outlet before the nerve damage becomes permanent.
Structural correction today is the only proven way to avoid the surgical table tomorrow.
Why Your "Hand Numbness"
Keeps Coming Back
You've tried wrist splints, TCM Tuina, and B-vitamins, but the "electric" tingling in your fingers always returns.
According to a comprehensive review by Harvard-affiliated researchers (Jones et al., 2019), identifying Thoracic Outlet Syndrome is exceptionally complex because it mimics so many other upper extremity conditions. Because it is routinely missed in standard differential diagnoses, patients are frequently left bouncing between failed treatments while their nerve irritation worsens.
The "Invisible" Compression
Most treatments fail because they treat the arm as an isolated limb. Your neck and shoulder act as the "Main Power Line" for your hand.
🔴
The "Strangled" Nerve:
Your nerves are being compressed in the Supraclavicular Zone. No amount of wrist massage can fix a pinch under your collarbone.
🔴
The "Biological Splint" Trap:
Your neck muscles (Scalenes) are tightening to protect a misaligned spine. This creates a "Biological Splint" that clamps down on your Brachial Plexus.
🔴
The "Double Crush" Failure:
Think of your nerve pathway like a garden hose. If it gets kinked in two different places, once at the base of your neck and again at your shoulder or wrist, the water stops flowing. If a practitioner spends months only massaging your wrist or stretching your shoulder, they are only fixing the lower kink while the main block up in your neck keeps strangling the nerve. To get lasting relief, you have to unkink the hose from the very top.
🔴
The "Pec Clenching" Executive Habit:
In high-pressure CBD environments, stress causes subconscious chest tightening. This pulls the collarbone down, creating a permanent mechanical "clamp" on your blood vessels.
🔴
Fake Carpal Tunnel:
Fake Carpal Tunnel: If your pinky is numb, it’s not your wrist. It is likely Arm Numbness & Tingling originating from a pinch in your shoulder or neck.
You shouldn't have to live in fear of "permanent damage" when correcting the structural "pinch point" can restore full nerve flow to your hand.
Beyond the Wrist: Avoiding the "Surgical Nightmare"
If you’ve been treating your wrist for months with no progress, you are "treating the victim".
The "Stroke" Scare
That sudden coldness or "buzzing" in your left arm leads many to the A&E, fearing a heart attack. Usually, it’s the Subclavian Artery being compressed at the collarbone.
The Surgery Fear
You may have seen scary videos of "1st Rib Resection" surgery. Most TOS cases in Singapore are mechanical and can be resolved by increasing the structural space, without a scalpel.
In Singapore, TOS is the most common misdiagnosis for hand pain. If you've been "managing" Carpal Tunnel for months with no progress, here is why:
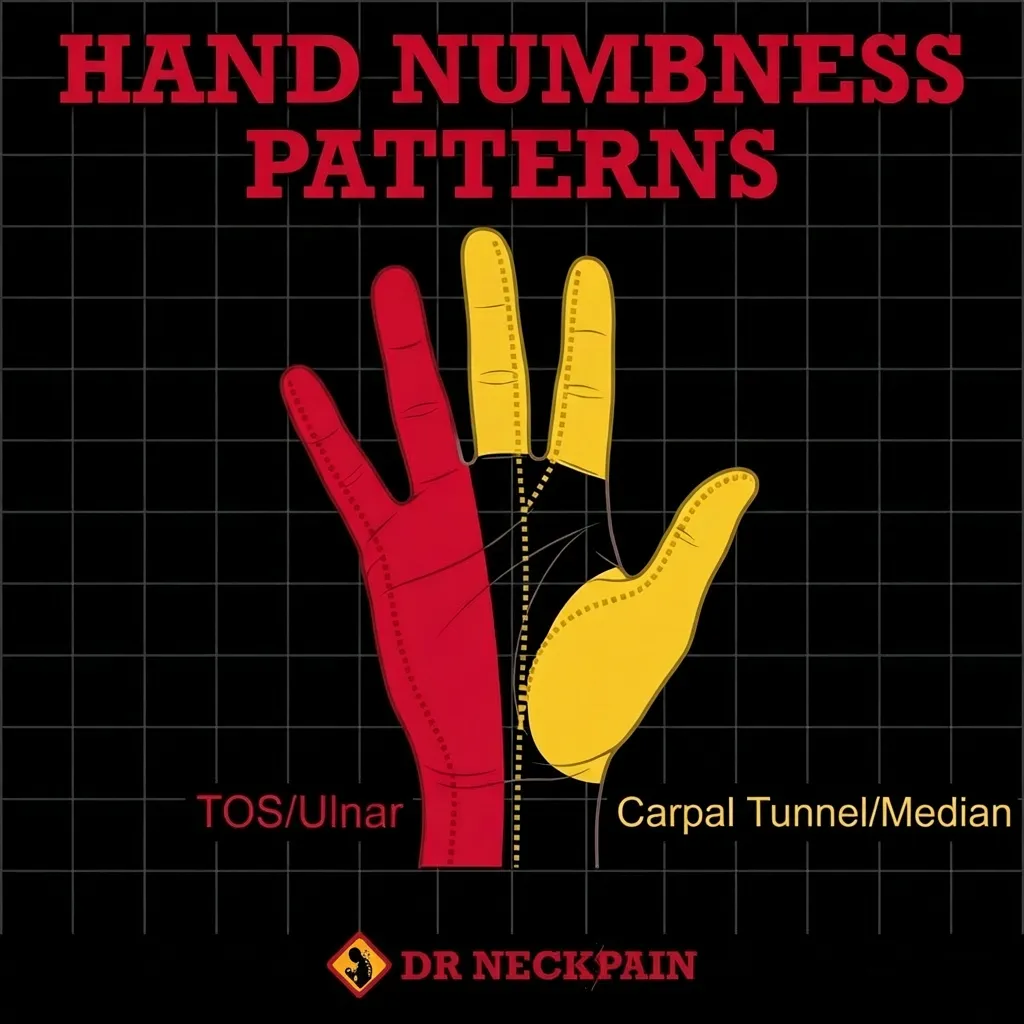
TOS / Ulnar
Carpal Tunnel / Median
The Stress-Breathing "Noose": Why Your "Tight Shoulders" Are Actually a Respiratory Crisis
Have you ever wondered why your neck tightness returns just minutes after a massage?
In Singapore’s high-pressure corporate environment, most professionals are "chest breathers." Under stress, the body stops using the diaphragm and begins to rely on the scalene muscles in the neck to lift the ribcage.
In clinical terms, this is known as Secondary Respiratory Muscle Recruitment.
The 22,000 "Mini-Shrug" Problem
The average person takes approximately 22,000 breaths per day. If you are a chest breather, you are performing 22,000 repetitions of a neck-shrugging exercise every single day.
The Biological Consequence:
Scalene Hypertrophy
Overworked muscles become thick, scarred, and "overgrown" (Ref: Kaplan et al., 1996).
The First Rib Elevation
These muscles physically pull your first rib upward, narrowing the gap between the rib and your collarbone.
The Nerve Strangle
This narrowed gap creates a mechanical "noose" that strangles the Brachial Plexus nerves and the Subclavian artery.
‼ The Specialist Verdict
You aren't just "stressed"; you are physically strangling your nerves with every breath you take at your desk. No amount of massage can fix this because the problem isn't the muscle; it’s the mechanical position of the rib and your breathing pattern.
Why Standard "Stretching" Fails
If you have Scalene Hypertrophy, stretching can actually make the pain worse. Pulling on a nerve that is already being "strangled" by a thick muscle only increases inflammation.
Our R3NEW X™ program focuses on Structural Decompression, resetting the first rib to its rightful place and "opening the noose.
Jones et al. (2019) confirms what we see clinically every day: relying on generic therapies or waiting it out is a degenerative strategy. The moment upper extremity numbness sets in, passive management is no longer an option. Timely, structurally targeted decompression is non-negotiable to restore neurological flow and halt the cascade before progressive mechanical failure leaves you facing surgery. Once that pressure is off, we safely transition to retraining your breathing mechanics.

The "Three Tunnels" of Compression
Your nerves and blood vessels travel through three narrow "tunnels" from your neck to your fingertips. At our North Bridge Centre clinic, we identify which tunnel is failing:
The Scalene Triangle
The "Fuse Box" in your neck
Where tight muscles clamp the nerves.
The Costoclavicular Space
The narrow gap
Between your collarbone and your first rib.
The Pec Minor Tunnel
The "Front Door"
Of your shoulder that shuts tight when you slouch over a laptop.
PSEUDO-ANGINA
The "Heart Attack" Mimic
Have you rushed to the A&E with chest pain and left-arm numbness, only to be told your heart is "perfectly fine"?
Many of our patients come to us after a terrifying experience. They feared a heart attack, but their EKG and blood tests were clear. This is a documented medical phenomenon called Pseudo-angina (Ref: Sussman et al.).
When the nerves in your Thoracic Outlet are compressed, they send "error signals" to your chest wall (the Pectoral muscles). This creates a sensation of tightness and radiating pain that feels identical to cardiac distress.
‼ IMPORTANT
Chest pain is a medical emergency. You must always rule out cardiac issues with a GP or Cardiologist first. If they have given you the "all clear" but your pain persists, we specialise in identifying the structural "short circuit" causing the mimicry.
The Solution
Clear the "Invisible Pinch": Reopen the Tunnel and Avoid the Knife
I know the frustration of "normal" scans when your hand is physically "buzzing", and your grip is failing. It’s exhausting to wake up at 3 AM to shake life back into a "dead arm," wondering if you’re facing permanent nerve damage. You may have even seen scary videos of "Rib Resection" surgery and feared that an invasive operation is your only option. Whether you're worried about your performance at work or simply want to carry groceries without your arm turning cold and heavy, that uncertainty is a heavy burden.
29 Years of Experience
In 29 years of clinical practice, 20 in Singapore, I’ve specialised in solving the "Invisible Pinch" that standard tests miss. While others treat the wrist, I focus on the Brachial Plexus, the "Main Power Line" at the base of your neck. Using the R3NEW X™ Program, we move beyond "still" scans to perform a functional audit of your Thoracic Outlet.
Structural, Not Symptomatic
We use forensic X-ray analysis to find the millimetric shifts in your first rib and collarbone that are "strangling" your nerves. We don't just rub the shoulder; we physically increase the mechanical space in the Supraclavicular Danger Zone.
By resetting the "Hinge" (the bone), we allow the "Cable" (the nerve) and the "Pipe" (the artery) to flow freely again.
Benefits
What to Expect from Our Structural TOS Recovery
Most treatments in Singapore only "mask" the symptoms of nerve compression. The R3NEW X™ Protocol aims for a permanent mechanical resolution by reopening the "Triple Tunnels" and restoring full neurological flow to your hand.
Restore "Weightless" Arm Mobility
Eliminate the "Heavy Lead" feeling. When the space between your collarbone and first rib collapses, every movement feels like you are fighting against gravity. By restoring the architectural height of your Thoracic Outlet, we "lift the weight" off your shoulder. The result? You can reach for high shelves, wash your hair, or hold the MRT grab pole without your arm turning cold or heavy.
Reclaim Precision Grip & Hand Function
Stop the "Ghost Numbness" and muscle weakness. When your Brachial Plexus is no longer being "strangled" at the neck, the "power lines" to your hand are fully restored. This means an end to dropping your phone, struggling with a mouse at your Raffles Place office, or the "pins and needles" in your pinky and ring fingers. You regain the fine motor control needed for your career and daily life in the CBD.
Deep, Uninterrupted Sleep (The 3 AM Reset)
End the cycle of the "Dead Arm" wake-up call. Many TOS patients spend their nights tossing and turning, unable to find a position that doesn't trigger a "Short Circuit." By resetting the Structural Hinge in your neck and shoulder, we calm the nervous system. You can finally sleep through the night without having to "shake life back" into your hand at 3 AM.
THE Process
The Structural Nerve Decompression Method: From Compression to Total Freedom
The Forensic Architectural Audit
We use a precise, medical-grade methodology to physically reopen the "Triple Tunnels" and restore your nerve flow by performing a supraclavicular evaluation, including a few orthopaedic tests, to determine which structures are involved. We map your Referred Pain Pathways so we never have to guess.
R3NEW X™ Correction
RELEASE
Using the AxisFlex Protocol™, we break deep fascial adhesions and "traumatic guarding" in the scalene and pec minor muscles. This flushes out the 'Energy Crisis' and returns oxygen to ischemic nerves.
RESET
We correct millimetric misalignments in your C7-T1 "Fuse Box". By resetting the structural hinge, we "lift" the collarbone, increasing tunnel volume.
RECALIBRATE
Through NeuroPosture Calibration™, we retrain your brain to maintain this open space automatically, even during 10-hour CBD workdays.
Full Function Restoration
Reclaim your grip strength and deep sleep. We provide objective proof of recovery with post-correction X-rays. You return to your career, your workouts, and your sleep.
Why "General Massage" is Ineffective (and Potentially Risky)
The Supraclavicular Zone (the area above your collarbone) is a high-traffic "Danger Zone." Clinical research confirms that the Phrenic nerve (breathing), Brachial plexus (hand function), and Subclavian artery (blood flow) are all crowded into a tiny, millimetric space.
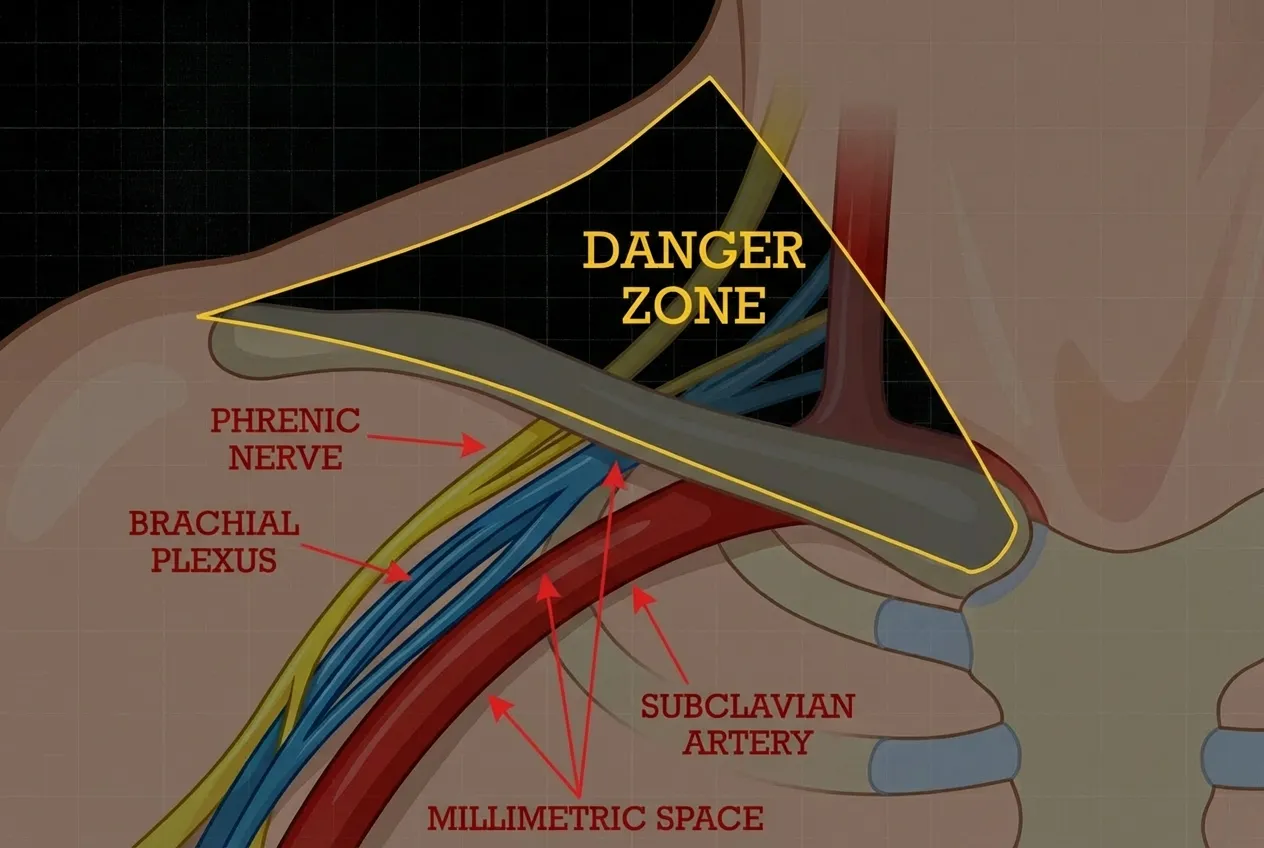
Why General Massage is Risky. The Supraclavicular Zone is a high-traffic "Danger Zone" where the Phrenic nerve, Brachial Plexus, and Subclavian artery are crowded into a tiny, millimetric space. Aggressive, "blunt force" massage in this area can irritate these delicate structures. True relief requires the precision of structural decompression to safely increase the tunnel volume.
⚠️ The Specialist Verdict
Massage is too "Blunt": General rubbing or deep tissue massage in this area is like using a sledgehammer for a watchmaker's job.
Irritation Risk: Aggressive pressure can irritate the Phrenic nerve or further inflame the already "strangled" Brachial plexus.
The "Structural" Reality: Massage cannot move a bone. If your first rib is jammed upward or your collarbone has shifted, rubbing the muscle will never create the millimetric space your nerves need.
Frequently Asked Questions about
Thoracic Outlet Syndrome (TOS)
Why are my pinky and ring finger numb but not my thumb?
Is Thoracic Outlet Syndrome a sign of a heart attack or stroke?
Can Thoracic Outlet Syndrome cause "Brain Fog" and Dizziness?
What is a Cervical Rib, and do I need surgery?
Why does my hand feel cold and look blue (Cyanosis)?
Why was my MRI or EMG reported as "Normal" if I have TOS symptoms?
Can I fix TOS with an Ergotune chair or a standing desk?
How is a TOS different from a Slipped Disc in the neck?
What is the "Gilliatt-Sumner Hand" and why is it a medical emergency?
Can Thoracic Outlet Syndrome cause "Brain Fog" and mental fatigue?
Why does my neck tightness return even after a deep tissue massage?
Can my smartphone really cause Thoracic Outlet Syndrome?
Stop Shaking Your Hand. Start Fixing the Source.
Join 3,000+ patients in Singapore who have solved the "Numb Hand Mystery," restored their grip strength, and reclaimed their sleep with X-ray-proven structural decompression.
You shouldn't have to "survive" your workday at Raffles Place by shaking out your arm every 20 minutes or live in fear that your hand will go "dead" during a big presentation. Whether you are terrified of losing permanent sensation or simply exhausted by the 3 AM wake-up calls, the problem isn't "just stress" or "too much typing." It is a mechanical blockage in your Thoracic Outlet.
Our R3NEW X™ Program is the precise, non-surgical solution designed to reopen the "Triple Tunnels," relieve pressure on your Brachial Plexus, and permanently restore blood flow and nerve signals to your hand.

Our 90-Day "Nerve Decompression" Guarantee
We stand by our work with a strict results-focused guarantee: We commit to objectively improving your functional mobility, reducing clinical nerve indicators, and significantly diminishing your numbness within 90 days, or we will refund your treatment fee. We track your progress using objective, post-correction structural benchmarks.
We don't just promise your hand will "wake up", we prove the structural change with post-correction X-ray imaging.
T&C Applies
The "Invisible Pinch" Analysis
Book your initial consultation, which includes a complete neurological history, provocative physical testing, and precise X-ray analysis to locate exactly where your nerves are being "strangled".
The "Structural Source" Verdict
We review your X-rays together to definitively show how your collarbone or first rib has shifted and to map out your 90-day restoration plan.
Neurological Freedom
Start your R3NEW X™ journey and experience the relief of an arm that feels light, warm, and fully "connected" again.
Expert Care for Thoracic Outlet Syndrome in Singapore
Conveniently located at North Bridge Centre, our clinic is the preferred choice for office workers and executives in Bugis, City Hall, and the Singapore CBD. Whether you are battling a "cold, numb hand" at your desk in Marina Bay or struggling with shoulder fatigue on your MRT commute, we are easily accessible for precise structural correction.
We understand the specific demands of the Singapore corporate lifestyle, the 12-hour "Desk Hunch," the high-stress environment of the CBD, and the ergonomic strain of dual-monitor setups. That is why our appointment slots and R3NEW X™ program are designed for maximum efficiency, allowing you to fit specialised nerve care into your lunch break without disrupting your workflow.
The Structural Approach
We don't just rub the numb hand; we fix the mechanical pinch point at the base of the neck. Our method restores the architectural height of the Thoracic Outlet, permanently eliminating symptoms.
Specialist Diagnosis
We find the "Cervical Rib" or "Fibrous Band" that standard hospital tests might miss.
No "Package Traps"
Results-focused care. We aim to decompress your nerves so you can get back to your life, permanently.
Private & Professional
A focused clinical environment suitable for high-performing professionals who need a real medical solution.
Find Us in the Heart of Singapore
📍 Clinic Address: 420 North Bridge Rd, #02-20 North Bridge Centre, Singapore 188727
🚇 MRT: 5-minute walk from Bugis MRT (East-West & Downtown Lines) or City Hall MRT Station
🅿️ Parking: Available at National Library of Singapore, Bugis Junction, and InterContinental Singapore
We are the trusted structural correction specialists for residents across the island:
Centre
Orchard, River Valley, Tanglin, and Newton.
Business Hubs
Tanjong Pagar, Raffles Place, Marina Bay,and Suntec City.
Heartlands
We frequently welcome patients from Tampines, Jurong, and Bishan seeking specialised TOS care not found in general GP clinics.
Clinical Research Vault: The Science Behind Thoracic Outlet Syndrome
Every recommendation at Dr Neck Pain Singapore is grounded in peer-reviewed research. Below are 15 published studies from The Lancet, Journal of Vascular Surgery, JNNP, Pain Therapy and leading medical journals, documenting why your arm goes numb overhead, why your MRI comes back normal, why wrist surgery fails, why TOS mimics a heart attack, and why conservative structural correction works.
Clinical References & Medical Sources
15 peer-reviewed studies: nerve compression, double crush, pseudo-angina, scalene anatomy, diagnosis & conservative treatment.
AJNR. American Journal of Neuroradiology, 33(7), 1247–1250. 👉 View Study
Journal of Applied Physiology, 93(6), 2109–2115. 👉 View Study
The Lancet, 302(7825), 359–362. 👉 View Study
Proceedings (Baylor University. Medical Center), 20(2), 125–135. 👉 View Study
Journal of Neurology, Neurosurgery & Psychiatry, 33(5), 615-624. 👉 View Study
Clinical Anatomy, 10(4), 250-252. 👉 View Study
The American Journal of Surgery, 132(6), 771-778. 👉 View Study
Indian Journal of Otolaryngology and Head & Neck Surgery, 76(4), 3532–3536. 👉 View Study
Archives of Physical Medicine and Rehabilitation, 78(4), 373-377. 👉 View Study
Pain and Therapy, 8(1), 5–18. 👉 View Study
Diagnostics (Basel), 8(1), 21. 👉 View Study
Journal of Vascular Surgery, 64(3), e23-e35. 👉 View Study
Joint Bone Spine, 68(5), 416-424. 👉 View Study
Journal of Athletic Training, 59(7), 683. 👉 View Study
Journal of Clinical Medicine, 10(5), 962. 👉 View Study